Intersex children in Kenya: The policy gaps behind early gender assignment
Across Kenya, intersex children are assigned identities at birth through decisions shaped less by law than by stigma, silence, and pressure. These early interventions, often irreversible, expose gaps in policy, healthcare, and accountability, leaving some of the most vulnerable navigating systems that were never designed for them.
At puberty, Hunielle Chivatsi (36) sat in a biology class, grappling with a growing sense that her body was different from those of her classmates. “I was different from both girls and boys my age. I began asking my mother questions, but she did not have answers.
“My father had disowned me at birth. Girls my age were already experiencing their monthly periods, but in my case, I did not. Whenever the school distributed sanitary pads, I would give mine to my sisters. I knew something was wrong,” she says.
At the time, she did not yet realise that her experience reflected a broader legal and medical dilemma in Kenya—one in which decisions about intersex children’s bodies are often made early, shaped by cultural pressure, limited medical guidance, and the absence of clear policy protections.
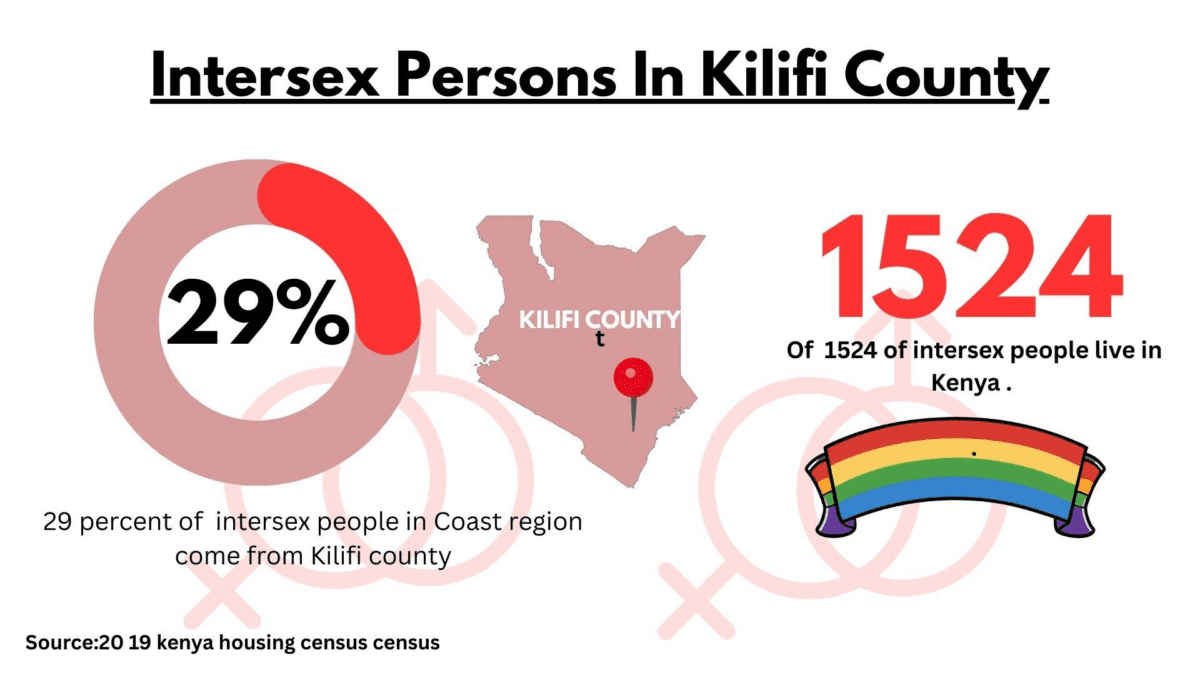
Her story is not an isolated one. According to the 2019 Kenya Population and Housing Census, Kenya is home to 1,524 intersex persons—individuals born with physical characteristics that do not fit typical definitions of male or female. While these numbers may appear small in absolute terms, their implications are significant. Each case raises fundamental questions about protection under Kenya’s Constitution, particularly the rights to equality, dignity, and health.
Yet despite this recognition in national data, intersex persons remain largely invisible in policy implementation and public health planning.
Forced identity
In the Coast region alone, 86 intersex persons have been identified, with Kilifi County accounting for 25 cases. Drawing from her work in the region, Hunielle says many intersex children are raised by single mothers and are often subjected to early gender reassignment due to community pressure—decisions that can later result in identity crises.
Sostine Lewa is one such case. A beneficiary of IRIC, she was born intersex at Kilifi Referral Hospital. Her mother died during childbirth, and shortly after her birth, her father authorised surgery to alter her genitalia—removing what he perceived to be male characteristics.
Decisions like these—often made by parents and medical practitioners in the absence of clear legal safeguards—highlight the lack of regulatory oversight surrounding gender assignment for intersex children in Kenya. “Intersex is a silent topic. Among the Mijikenda, children born intersex are considered kijego, meaning a curse. Many communities distance themselves from such children, viewing them as a bad omen or a sign of misfortune in the homestead,” she says.
Today, Sostine says she wishes her body had been left intact until she was old enough to make her own decision about surgery. “Looking back, I feel so sad. Perhaps I would have fathered children by now. No one disclosed the truth about my sex, and I was raised as a girl,” she says.
“I struggled to fit in. I got along more easily with boys, but I was expected to live as a girl. At puberty, I never experienced menstruation. I don’t know what it’s like to use a sanitary towel. When my nieces ask me to show them how to use one, I feel sad because I have never experienced it myself.”
Sostine only discovered she was intersex during an awareness session organised by the Intersex Rights Initiative Coast (IRIC). The revelation left her distressed and searching for answers.
“I called a family meeting and asked my father to tell me the truth. He cried and admitted that I was born intersex. But because the community saw it as a curse, he chose surgery as a way of protecting me,” she says.
Her experience has shaped her view on parental decision-making. “Parents should not choose the gender of their intersex children. They should allow them to decide when they are adults,” she adds.
Bridging gaps
Founded in 2023 by Hunielle Chivatsi, IRIC is a grassroots organisation based in Mtwapa, Kilifi County, that advocates for the sexual and reproductive health and rights (SRHR) of intersex persons. It also works to rescue and support individuals who have been abandoned or marginalised due to their intersex status.
Between 2024 and 2025, the organisation supported five mothers and their intersex children who had been abandoned by their families, providing shelter through partnerships with other stakeholders. It has also created employment opportunities for 15 intersex individuals and reached more than 200 people through community dialogue.
Beyond these direct interventions, organisations like IRIC often step in where formal systems fall short—bridging gaps in healthcare access, legal awareness, and social protection for intersex persons.
“Addressing the sexual and reproductive health and rights (SRHR) of intersex persons is extremely challenging due to physical variations, compounded by stigma and the lack of appropriate medical equipment,” Hunielle says.
“It is these complexities that motivated me to start the organisation. In the coastal region, there was a clear need for better SRHR services, a rescue shelter, and a centre for inclusion.”
An intersex awareness survey conducted by IRIC in Kilifi received 498 responses. It engaged more than 50 stakeholders, including police officers, religious leaders, village elders, and cultural leaders—many of whom are key decision-makers within the community. The findings highlighted the multiple layers of challenges intersex persons face, including those linked to religion.
“I wanted to address the issue of religion. As a Muslim, I am often unsure where to pray—women see me as a man, and men see me as a woman. This showed me the need for dialogue, so people can understand that religion goes beyond physical appearance,” she says.
These lived experiences are unfolding against a backdrop of ongoing legislative efforts aimed at addressing such gaps. The Intersex Bill 2023 seeks to respond to persistent human rights violations affecting intersex persons in Kenya, according to the Kenya National Commission on Human Rights (KNCHR).
Among its provisions, the bill proposes formal recognition of intersex as a third gender and requires that children born intersex be issued with official birth documentation reflecting their status. However, Hunielle notes that the absence of an enacted legal framework continues to limit the effectiveness of grassroots interventions.
“The lack of this law makes it difficult for organisations like ours to meet our objectives fully,” she says. “There is also no clear legal guidance for parents who assign gender to intersex children at birth.”
This gap extends beyond national policy. Advocates like Hunielle increasingly frame their work within broader continental commitments. Under Agenda 2063 and the African Union’s Gender Equality and Women’s Empowerment Strategy, member states—including Kenya—have committed to principles of non-discrimination and bodily autonomy.
In that context, gaps in civil registration systems and clinical protections for intersex children are not only national challenges, but also raise broader accountability questions within Africa’s human rights framework.
Yet even beyond the legal and policy space, structural challenges within the health system persist. “Right now, there are no suitable sanitary products designed for intersex persons in the market. Even in cases like cervical cancer, public hospitals lack equipment that accommodates intersex patients for proper screening,” she adds.
Medical perspective
At the same time, medical perspectives within the health system continue to shape early decisions about intersex children—sometimes reinforcing, and at other times challenging, societal pressures.
Dr Kalama, a paediatrician at Kilifi Referral Hospital, advises that parents of intersex infants should seek specialised medical guidance, including consultations with paediatricians, endocrinologists, and geneticists. “Physical appearance alone is not sufficient. Genetic testing can help determine a child’s chromosomal makeup and guide medical understanding,” he says.
Dr Fondo adds that such tests typically identify whether a child has XX or XY chromosomes, which are associated with female and male biological patterns, respectively. “If a child has XX chromosomes, they are genetically female at the cellular level, with a predominance of female hormones and internal reproductive structures such as ovaries. If the child has XY chromosomes, they are genetically male, regardless of external appearance, and will typically develop male hormonal patterns,” he explains.
He notes that internal reproductive organs may not always be externally visible and can be located within the body.
However, Dr Fondo cautions against early surgical intervention. “Parents should avoid making irreversible decisions in infancy. Proper medical evaluation should come first, and decisions should not be driven by social pressure,” he says.
He emphasises that surgical procedures should be considered a last resort and only after thorough medical consultation.
Akinyi* (not her real name) knows firsthand the consequences of stigma and misinformation. After giving birth to an intersex child in mid-2024, she was met with silence and suspicion at the hospital.
“Immediately after delivery, they took my baby away without showing me. They said they had called my mother-in-law,” she recalls. When her mother-in-law arrived, the reaction was harsh. “She looked at the baby and asked why I had brought a curse into the family,” Akinyi says.
Within days, her husband took a second wife and forced her out of their home. Akinyi later found support through IRIC, where she received counselling and guidance on raising her child.

Stigma in schools
Hunielle is advocating for a multi-agency approach to address stigma and create safer, more inclusive environments. Her organisation works closely with parents, particularly mothers, to help them accept and support their children.
“We encourage parents not to rush into surgery. Many had lost hope in their children, but through engagement, we have helped restore that hope. Some children had been hidden due to shame,” she says.
“I was raised as a girl, but many people did not understand me. Even now, some believe I am a woman, while others say I chose to become a man,” Hunielle says. She adds that intersex persons remain undercounted, noting that official statistics may not fully reflect reality due to low awareness and stigma.
Hunielle’s own experience reflects the barriers intersex individuals face within the education system. When her family relocated, she was denied admission to a primary school because of her physical appearance.
“My mother took me to a new school, but the headteacher looked at me and refused to admit me without explanation,” she recalls. Even after securing admission elsewhere, she struggled to navigate gendered spaces.
“I started schooling in trousers, but I was still uncomfortable. When I went to the boys’ toilet, my classmates expected me to stand, yet I had to squat. They did not understand, and I felt exposed,” she says.
In response to these challenges, IRIC has developed targeted interventions that engage both community actors and institutions.
One such initiative is the Muramuko (“awakening”) project. It works with key community figures—including Community Health Promoters (CHPs), police officers, village elders, wazee wa nyumba kumi, security guards, and boda boda riders—to build awareness and shift perceptions.
“We work with these duty bearers because they influence how communities think. We also collaborate with hospitals. When an intersex child is born, health workers call us, and we engage the parents,” Hunielle explains.
The Fimbo project focuses on schools, engaging teachers and management in dialogue around inclusion. “We encourage schools to create safer environments by moving away from rigid gender classifications—for example, using unlabelled toilets instead of strictly male or female ones,” she says. The initiative also uses social media to reach young people and expand awareness.
Another programme, Utamaduni, engages different cultural groups to explore how intersex identities are understood within various traditions. “It brings together different communities to reflect on what it means, culturally, to be intersex,” Hunielle adds.
Fragmented efforts
Jane Nyambura, Head of Programmes at IRIC-Kenya, highlights a significant funding gap for intersex-focused initiatives in Kenya. “Reduced support from Western donors has affected our programmes. We need the government to allocate resources for intersex awareness so we can reach more communities,” she says.
This reflects a broader structural issue: limited domestic investment in intersex rights programming, leaving organisations heavily reliant on external funding. “We currently depend almost entirely on international donors. With funding dynamics shifting, including the withdrawal of support from agencies like USAID, this is becoming a major challenge,” she adds.
Despite these constraints, IRIC’s advocacy has led to visible changes. Several facilities in Mtwapa have removed gender labels from public spaces such as toilets, making them more inclusive. “These changes show progress. Some public hospitals have already done away with male and female labels in certain areas,” Nyambura notes.
She is now calling for similar reforms across government institutions and schools to better accommodate intersex individuals. Intersex rights, like other fundamental human rights, are recognised in Kenya’s Constitution and supported by various legal frameworks that prohibit discrimination and violence. However, activists argue that legal recognition alone is insufficient to address deeply rooted social practices.
The persistent belief that all individuals must fit into strictly defined male or female categories continues to drive stigma and exclusion. In some cases, this has led to medically unnecessary surgeries and other invasive interventions on intersex infants and children without their consent—practices that have been condemned by international human rights bodies.
Several institutions and organisations have sought to address these gaps, though efforts remain fragmented and uneven across regions. The Kenya National Commission on Human Rights (KNCHR), alongside other human rights organisations, has been leading advocacy efforts to support intersex persons, particularly in the coastal region.
Other key actors include the Association of Intersex Parenthood (AIP), which works to support and empower intersex individuals and their families, and the Intersex Persons Society of Kenya (IPSK), a grassroots organisation focused on advancing awareness and rights.
However, stakeholders note that these interventions have lacked consistency and nationwide reach. Many are calling for a stronger presence at the county level to ensure sustained impact.
Frankie Kibagendi, Executive Director for intersex programmes at Jinsiangu Kenya, emphasises the need for policy implementation and grassroots awareness. “In many villages, local leaders and government representatives do not fully understand what it means to be intersex,” she says. “Without that understanding, policies cannot translate into meaningful change.”
Kibagendi is also urging the government to fast-track the passage of the Intersex Bill 2023, arguing that its absence continues to perpetuate exclusion. “The lack of legal recognition creates barriers, especially in documentation. Even in electoral processes, there is no provision for intersex persons, forcing them to identify as either male or female,” she explains.
She adds that, despite the 2019 census recognising intersex persons, there has been limited visible progress in translating that recognition into tangible support at the community level.
Until these gaps are addressed through clear policy frameworks, sustained funding, and institutional accountability, intersex children will continue to navigate systems that are not fully designed to recognise or protect them.
Leave a Reply